
How to Optimize Your Iron & Copper Levels, Oxidative Stress, & Peak Health with Dr. Rick Cohen & Dr. Fiona Chin
The below is a summary of a recent discussion between Rick Cohen, MD, and Fiona Chin that delved into various health-related topics such as iron levels, iron dysregulation, copper, mitochondria function, and chronic diseases. Dr. Rick Cohen highlighted the risks associated with excess iron causing harm due to oxidative stress and emphasized the importance of understanding iron dysregulation. Misconceptions in managing iron levels, markers for assessing iron status, and strategies for managing iron levels effectively were thoroughly explored during the meeting. Dr. Fiona Chin and Dr. Rick Cohen underscored the significance of iron regulation, inflammation, and oxidative stress on health, advocating for a holistic approach in addressing iron-related concerns.
The simply summary is find the cause of your iron problems rather than just randomly treating it. You must find out why the problem is there first! Low iron inside the body may also be a symptom of iron dysregulation more often than not caused by an iron and copper imbalance inside the body. Low iron doesn't necessarily mean it's time to take an iron supplement or up the dosing if it is not working; in fact, taking more iron may cause your problem to get worse. Ferritin is mostly an overused and unhelpful marker. Giving blood is a simple solution to consider for high iron but first to be discussed with your doctor. Get more info below or read more blogs here.
RICK Yeah, so I'll kick things off about discussing Morley Robbins, the iron guy (our MLP Formulary is based off his research). You need to have him on. Morley's been studying iron copper for twelve years, hours a day, and he's still learning new things. So there's a small percentage of people who really understand this, what we'll talk about. But there's some red flags that people need to be aware of, and there's some things that are being done in a number of people's opinions incorrectly and, you know, actually harming people.
FIONA It's so interesting with the copper. Like, I see this debate on the naturopathic pages here all the time with people that we're anemic, and then some people have done more ease. I think you must have a course of training. And so people bring that up, and then the standard naturopathic thing doesn't agree. If you're low in iron, you must take iron....
FIONA Let's take a step back and learn more about Rick Cohen before we get started. Rick is a functional physician. He's been in medicine for 25 plus years. He's the founder of the Ignite Longevity program. And actually, it's a company that provides personalized assessments and integrative interventions to help people will take a comprehensive approach to living longer, healthier lives. And he's dedicated his career to the treatment and prevention of lifestyle and metabolic related diseases. So his goal with patients is to really help them unlock the key in achieving optimal metabolic health. As a physician, he strives to educate those who are ready and willing to commit to living a full life. One of the amazing things that Doctor Rick Cohen is very well versed in is the relationship between iron, minerals, copper and all these amazing things and the role that they play in chronic disease, metabolic disease and kidney disease. And it's something I know even as a naturopath, you know, we're taught low iron supplement iron. It's as simple and as easy as that. And then look for the cause. You've probably got some food allergies or some parasites, and that's probably, you've got a heavy menstrual bleed if you're a female, and it's really that simple. But as Doctor Cohen is going to take us on a journey today, it's really not that simple. And of course, our beautiful kidney disease patients are often chronically low in iron due to this EPO link. So, Rick, thank you again for coming on the YouTube channel and sharing your knowledge with us. This is a really interesting topic for me, and one, I'd be lying if I said I know the basics, but I don't know all these other intricacies that I think are really important that we educate our community about. So thanks.
RICK Yeah. So this is a super interesting topic. And just how you led up to it used to be. And the same thing for me, this is easy. Your iron deficient or you're not quite iron deficient, because iron helps key some particular enzymes and deliver oxygen. Maybe you should take some because it'll help improve performance or energy or whatever it might be. And I will say, oh my gosh, I was 100% incorrect, or miseducated, or dis educated, or misinformed, whatever it might be. And while I was always aware of the problem of high iron and going back as part of 25 years ago, I had a cardiovascular screen, which one of the things was checking for iron, although I was checking the wrong marker. I'll talk about that. I was checking ferritin, which is what we'll go over this and not paying attention to the real markers. I wasn't aware of the critical importance and it's just something that was never really taught to the level that I became aware of when I was sort of educated and mentored by a researcher who's been down this path for twelve years a day. Achieving a certain level of health requires an individualized approach as well. What I can do, what I need, what I can do, and then what I need to check for me because we are all different.
RICK Point number one is to know where you are, even if the pathology is the same. Even if western medicine has deemed you all have kidney failure. But, you know, as you know, I'm sure you talked about, there's many different reasons for that, right? So just because you have a pathology, what's causing it, and if, you know, if you don't treat or figure out what the cause is, then you're really never going to get to the cure or the control. You're just band aiding the problem. But that's how western medicine works. It band aids the problems with a pharmaceutical or an interventional model. Hopefully this one little snippet of what we can discuss about iron, copper, vitamin a, magnesium and ultimately mitochondria. And the things to be aware of that you can do easily and look at in basic serum chemistries for the most part to guide you at least to say, whoa, maybe I don't need iron. Maybe I should try some copper or some vitamin a or something else first.
FIONA Fascinating. I'm also taught to look at ferritin. And I'm not sure what reference ranges you measure in the US, but in Australia, we look for a ferritin sitting over 50 and then iron to be in a sort of regular range. But ferritin is the most important marker, really, on the iron test that we get told. And then you're looking at, you know, total iron volume capacity and all those sort of things, you're making sure that iron's not too high. I mean, we do take that into consideration, but if your ferritin's below 50 and your irons on the low side bank strikes straight away, you need to go on an iron supplement if it's really low. Maybe you've got a gut parasite, maybe there's a food allergy causing microblading, or do you have endometriosis? Really heavy bleeding if you're a female. And we look at it that way, and that's really for the bulk of naturopathic medicine.
FIONA: Tell me why that is so wrong.
RICK It's so wrong.
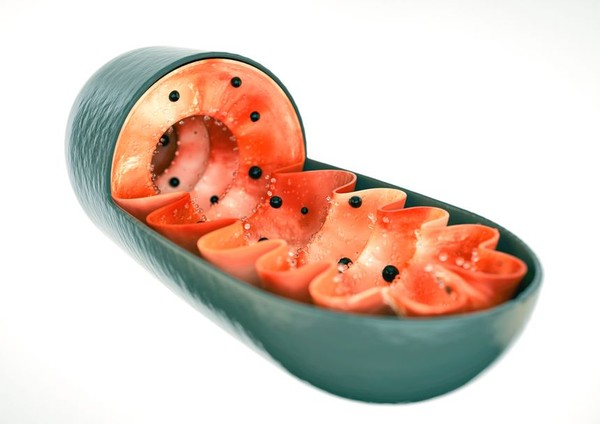
RICK: Let's start with energy, right? And why are we alive? Right? We're alive because we have these little batteries or these little foreign bacteria, organisms called mitochondria, which found our way into our cell and decided to coordinate with one another through these bioelectrical signaling molecules. So we have this organism of cells that sort of work together. It's quite. That's a whole other discussion about cells. No, how cells signal one another. Not related to our genetics. And it's a little bit off topic, but, you know, if you take. They have a way of telling each other on what to do, and it's a work of Michael Levin.
RICK And if you want to just get blown away, you know, Michael Levin's podcast with Lex Friedman, or in any variety of ways. And he talks about how cells like a skin cell and embryo, if separated, will become a completely different organism. It's like letting a kid out of kindergarten and he doesn't have the teacher around anymore, and he's just gonna go crazy in the store or the candy shop. The cells are controlled through this coordination, which are energized through mitochondria. The more active a organ is, the more mitochondria. The cells within those organs have, you know, the brain, the heart, the ovaries, you know, they have tremendous, much higher levels of mitochondria because it needs to produce more energy.
RICK: And then the mitochondria are really important for stem cell production. And if you begin to lose energy production in the mitochondria, you can't repurpose or expand your stem cells, and those fizzle out, and you're done. So just to give you a sense, there's some research being done now with actually bioreactors of mitochondria, where you transplant mitochondria and they find their way into the cells, and you're just sort of reloading your battery of the cells. Right. So really cool, really cool stuff topic for another conversation, for sure.
RICK So how do we create energy? Right. Well, two things. More than two things, but two major things. What do we need?
RICK: We need oxygen. And we need basically carbon. From food, from either fat or glucose, primarily. Right. And that through chemical reactions, you know, there's the Krebs cycle and then there's the electron transport cycle. And I'm not going to go into that details. There are people we should spin that on, but actually, that's the process. Now, that electron transport chain in the mitochondria is just literally, it's moving electrons in and out of the mitochondrial membrane. And there's five little complexes that actually have colors, and that's how they were first discovered. The fourth and the fifth one are the most important for sort of creating energy. And it's in that fourth one where sort of the magic happens, and that's where iron and copper need to interact.
RICK: So the warm up is iron and copper! They work with one another to create energy. And this is because hundreds of millions of years of maybe a billion years ago, the planet was anaerobic, which means we had a planet that had no oxygen. It was like 1% oxygen. So it was a planet dominated by iron. Right. So what happens with iron and oxygen?
FIONA: It rusts.
RICK: It rusts, right. Well, the rust that we see when you have iron and oxygen. So we needed to deliver. Now, when oxygen, when there became more oxygen in the world, more plankton in the sea, all of a sudden it reached a threshold. And 99 point something percent of the life on planet Earth died off. The organisms that were able to adapt because they were able to use copper to handle the oxygen. There's a shuttle between iron that is rustable or oxidized versus copper. They both have two and three electrons we won't get too much into the science there, but it needs to be a handoff between those two. And it's copper that allows iron to do its job and not to rust in our cell or not to create reactive oxygen species. Okay?
RICK: That's an oxidative stress, antioxidants, and so forth. The analogy I like to use is we want our mitochondria to be like a tesla, right? We want it to be this powerful engine driven. You know, this powerful engine that drives this car up a hill really quickly with no exhaust. Okay? That's a highly efficient mitochondria. It's producing energy. It's spinning off just a little reactive oxygen species. It's got enough copper. It has its cellular protective antioxidants. The membrane is healthy and so forth, and it handles it. Our body knows how to do that. When there's too much iron and there's not enough copper, these mitochondria become more like a diesel truck going up a steep hill. It can have a really big engine, but it's spewing diesel exhaust, and that's. That's the oxygen species, and it's the fatigue and it's the poor
RICK: Many people's mitochondria are spewing off oxygen, at risk for damage from free radicals. And to me, that's the endurance athlete who's not taking care of their mitochondria. They may have a lot of mitochondria, and they're really fast and powerful, but they're creating all this waste product and eventually doing themselves harm and damage. So, you know, having a VO two max, necessarily, that's high. But not understanding the efficiency of the mitochondria can be misleading. So while it's good to have a big engine and it's good to have mitochondrial density, having a big engine can be actually harmful, because on the flip side, you can also have, like, a little four cylinder Honda that doesn't go very fast up the hill, but it's still maybe it's a hybrid and it's not spewing out right. So even though it's not as powerful, it's more efficient and it's clean.
RICK And that's sort of what metformin can do for Berberine. It affects the first cytochrome, so it actually throttles down the mitochondria. So it's sort of like taking that engine and said, you're not going to go that fast. We're going to give you a smaller engine in your car, and because now you have a smaller engine and it's a little more efficient, you're not going to make as much reactive oxygen species, you're not going to cause as much damage to the iron. It doesn't need to process as much energy. It's that sort of analogy to think of on the mitochondria. So our goal is to have a really efficient, powerful mitochondria. But first is efficiency is not to spew out.
RICK That happens, like I said, when we have too much iron and not enough copper to handle that free electron that needs to be spit out, you know, in the process of creating energy. So that, that's, that's sort of the vision within it. And then it gets a little bit more like there's the fifth electron chain, which has to do with magnesium. And if there's too much stress or there's not enough magnesium, then you still don't create energy, you know, so there's those need to come into play as well. And I guess while we're talking about it, you know, the. That for cytochrome, it's not. It's copper, but it's really this molecule called ceruloplasmin, which Morley talks about it as this big molecule, and it's a transformer.
RICK It has many different shapes that it can transform itself in the body that needs to be loaded with copper to be efficient. Right. And in order to load copper, you need vitamin a, natural sources of vitamin a, to get that job done. So a lot of times, if you're deficient in vitamin a, you can't load copper into suroplasm. And suroplasm doesn't work, or vice versa. In today's world, a lot of the foods are copper deficient due to the type of farming, due to synthetic nitrogens, due to glyphosates, due to certain antibiotics, they all chelate copper. So just so glyphosate is, which is monsanto or bare now. Right? So we know it was first developed as a chelator. So it was a chemical. It was a chelating agent. And a chelating agent chelates minerals. What is one of the minerals it primarily chelates?
FIONA: Copper
RICK: Yes, Which you're depleting the foods of copper, you and beef liver. So copper is stored in the liver, but beef liver today has like 70% less copper in it than it had 30 or 40 or 50 years ago. So it doesn't all. Yeah, it's being depleted. So now we have decreased copper and you have a world where at least in the United States, they add iron to grains and cereals.
FIONA: So we're causing basically oxidative damage inside the cells.
RICK You're just creating oxidative damage! I go, how did they not know this? You know? Or do they know this? Someone knows? Or is it just like. It's just, you know, the world going in a particular direction? It just seems to happen. But just every decision that seems to be made seems to head in that direction of creating more oxidative stress and more damage in the population. And it's quite frightening because, you know, one hand, like, who knows this? Because they know from the physicians I know, even the more longevity focused ones, they're not aware of this. No, there's a few researchers that do and morally knows it. I don't know who knows this.
FIONA So my next question then is, well, why then is iron deficiency such a thing? Because it's probably one of the most common deficiencies we see. So people will be like, well, hang on a minute, though. When I have my blood tests, I'm always, and I'm one of these people, I'm chronically iron deficient, even though I eat red meat.
RICK Let's go to that. Okay, so we painted the picture and we won't go any deeper than that. Mitochondria, energy production, iron and copper protecting, being important in the key state of energy. Copper being deficient, iron excess due to all sorts of reasons. And the one. One thing I'll mention other than women who bleed regularly, and what happens is women in menopause, their iron levels go up and their risk of disease also increases. Women bleed regularly, so they tend to be less likely to have iron problems while they're considered irregular bleeding. In the modern world, we no longer have something you said before, parasites in the developing world, pre modern world, we had helminths and hookworms. So we had this symbiotic relationship with these parasites, which what they do, they bled us.
RICK So we had natural bleeding. So our iron levels, which as men, you can't get rid of. So if you're taking extra iron, it just builds and builds and builds. We won't do the math here, but if you figure out what you're getting every day and what you lose, because you only need a milligram a day to recycle to create red cells. You have like 2030 extra years of iron in your tissues. So let's think about that. If this is what you're eating, and you're eating this much iron, where is it going? It's going into your tissues. Here's the second piece. It's not iron deficiency, it's an iron dysregulation. So it's the iron being bound in the tissues which is now not available to be used to create the red cells.
RICK And going back to Otto Warburg and Krebs, what they found out was they actually bled birds. This is one of Morley's great stories, and it's in his book, they bled birds to Death. And then they looked at the liver and you know what enzymes popped up? Copper. It was like ten times the amount of copper related enzymes in seroplasm. Just exploded because the body was saying, holy, we have low in iron. We need to make more copper, you know, to make things and to get it out of the tissues, which, you know, and the old way is like you treated anemia with copper and vitamin a. That was sort of the awareness of it, because they sort of understood and we've forgotten that.
RICK I wouldn't even say maybe we've been misled, because we'll talk about ferritin, because we need to know what to pay attention to is iron is bound in the tissues and you need to get them out of the tissues. So let's talk about what should you look at? And it's so nuanced because iron could be in the liver and it has to do with ferroportin and hepcidin and all these sort of regulatory enzymes that allow input and block input. And the spleen plays a key role as well in the spleen, because that's where red cells are recycled, and iron can get trapped in there. We won't go there. But. But this is a cycle, so that's the other key point. Iron is cycled. Right. Since we only need 1 day, we just need to recycle it because we're building red cells.
RICK The red cells are used, they last three to four months. They get old, they get destroyed. We need to reprocess them, break them down into bilirubin, heme and carbon monoxide, actually. And then it reprocesses, you make new red cells. So what do we need to look at then is let's get back to what's important. The most important marker, you know, I look at is serum iron. Like, what's. What's in, what's in the serum and hemoglobin. So that was the old thing to look at, right. Hemoglobin is how much heme is the way the body's carrying iron. For the most part, 70% is in heme. Heme is just a protein with an iron clustered in the middle, and that gets packed into the red cells, which then take oxygen and deliver it to the mitochondria to be processed for energy.
RICK Somewhere, somehow, ferritin, which is a storage protein, but a storage protein in the tissues, and there's different types. There's a low density, a high density storage protein. And if you talk to the researchers, understand ferritin, the ferritin in the blood is really more of an inflammatory marker than a carrier of iron. And people know that, doctor. Well, it's an acute phase reaction. Yes, primarily, that's what it is. It's a marker of inflammation. Now, it can be very high when there's extra iron because there's inflammation, because iron is inflammatory. As you pull iron out, you can reduce inflammation. But it also could be high after doing a marathon. It also could be high after a virus infection. It also could be high with liver disease, fatty liver. So there's many things that will drive ferritin up.
RICK It also can be low if there's some spleen issues. If the spleen is not producing things, it could be artifactually low. One of the key researchers in this area said, technically we should have, we don't need ferritin in the blood. It wouldn't even come out at all. When we look at ferritin, 20 is a good number to have. I almost don't pay attention to it as a marker of high iron other than if it's coming up low. And let's get back to if hemoglobin, serum iron, and then iron saturation. So when you look at the CBC, red blood cells, right? So we need red blood cells to be floating around, but the red blood cells need hemoglobin in those with heme. So knowing that hemoglobin, it varies a little bit. Women have a little bit lower naturally, since they bleed and they're smaller, typically.
RICK And it varies. Men have higher testosterone drives hemoglobin because why? Because it's an mTOR driver. Right. Iron is also an mTOR driver because what do you need to grow? You need oxygen. Right. So, so if you're in anabolic state, your body needs more iron, and testosterone will cause greater absorption of iron. And it's. And if men know that, it's like, oh, I'm taking testosterone, my hemoglobin's gone too high. And they'll actually tell people to, you know, to give blood to. I tell people to give blood most of the time anyway, but that's like, well, okay, that's. So there's a downside to testosterone, too, from its longevity effects. If you don't pay attention to that extra iron being absorbed, you're sort of paying Peter to Paul, you know, borrowing Peter to pay Paul.
RICK You might benefiting one hand, but your long term effects are not good. So what we want to shoot for is we talked about parasites and not regular bleeding, or even you would get cuts and you would naturally bleed and lose some blood periodically. Typically an idealistic be on that lower threshold of hemoglobin. So women 13, man around 14. So I shoot for that lower part. You don't have to be there, but that's sort of a goal. As we start to optimize. Then you want to look at serum iron. Typically around 100 is, I don't know, the units off the top of my head, but 100 is the goal.
RICK And because you can have too high iron in the serum or too low, and each of those are an indicator of either excess iron or you still can have excess iron and low serum iron if it's in the tissues. So you really have to look at multiple markers, and then you have to look subjectively at the person. Have they been taking iron? They have an issue. It is not. It's very nuanced to understand this. The other piece that is important is iron saturation rate. So you have serum iron, and then you have total iron binding capacity, which is the protein that carries iron through the tissues. And just sort of like a bus that has certain amount of seats. You know, that iron saturation tells us of how overloaded or how crowded the bus is. We ideally want around 20%.
RICK I like to keep that low. You really want enough iron to make sure you're within that lower range. But, you know, keeping hemoglobin above normal, keeping iron saturation and serum iron around 100. And then at that point, if you're good, don't care about ferritin unless it's way high, and that's a sign of some major inflammation. Yeah, transferrin is sort of how they calculate is the protein that carries it. And, you know, a high transferrin can be a sign of parasites.
RICK So there is one of the nuances is also anemia of age, anemia of chronic disease. And I'll give you a personal story. My mother is twice now. Once she went to the hospital with a urinary tract infection and they had to give her iv's and she came in and her hemoglobin was fine. And, you know, I saw her blood work. Our caretaker sent it to me. And then, so, you know, three days later, after they gave her iv, she was feeling better and they said, we're going to send her home today, but we're just going to give her some iv iron. I'm like, what? Like what? Well, because she's iron deficient. I was like, no. And I, you know, it was already done. And I got on the phone, I was like. I asked, well, how.
RICK How did she look when she first came in? She was good. Does she have any signs of iron deficiency? No, everything was good. They didn't do everything, but her hemoglobin or CBC was good and they looked at ferritin, whatever. They didn't do iron such. We don't do iron saturation. Why? Because you don't want to know. But he said to me, this is the ER. It's like, well, we can't do anything with it. So since there's no action step that we would take, we don't bother looking at. All right, that's fine. So then three days later, she goes, oh, her hemoglobin was ten, so we need to give her iron. I said, I go, well, was she bleeding? No. You know, what did you give her?
RICK Chelating age. No, no. So where did the iron go? And he's like, couldn't answer it. And I tried to say this in a nice way. I said, I didn't know this. And I've been doing research for the past couple of years, and it's like, you realize that iron fuels bacteria and parasites, right? That's what they need to grow. So what do you think the body does when you're in a sense of infection? It says, we're pulling this iron away. It took the iron. Her body still knew what it to do at some level, put the iron in the tissues to help protect herself against infection, which she had. What they did was put the freaking iron back into her.
RICK They were going to feed the infection, which she had a problem with. And then they did it again after. And it's like this. So they just non paying attention with non thinking about what the body's mechanism is to do with iron and how I can just load the tissues. So we also see it. And I'll give you another. We work with some professional mountain bike cyclists, and they've all been told, oh, you know, I'm not writing so well. And they look at their ferritin and they're all 20 something, and, oh, your ferritin's a little low. Take iron. Okay. Well, guess what? They notice right away they feel better. They feel better right away, right. But this doesn't last.
RICK Then, well, and then we look, and their saturation rate is 50%. And it's like, hold on a second. Now you've become iron overloaded. And then when you look at their markers, they were actually magnesium deficient, copper deficient. You know, they were stressed out. They weren't handling their adrenals. But someone said, take iron, which is just like this minuscule short term fix, which made the problem worse. So what you'll do is like, let's donate some blood. And I will actually do that. Like, if someone is like, you know, one will evaluate them. And I'm not saying everyone does this, but it's like, you can go to the Red Cross, you know, in the United States, and they'll take your blood as long as you're good.
RICK So donate a little bit of blood. Right. Because sometimes donating blood gets things moving. And its a charitable thing to do as well.
RICK Right. So as you pull blood out, it starts to pull it out of the tissues, and you start to create some regulation. You have to be careful depending on someone's initial state of health. And sometimes you'll just say, pull 200. Normally it's at 500 mils, and you'll pull just a little bit just to get things going. And I hear all that, wow, I felt better, right? I feel better now. You'll see, like, the blood's thicker and it's really dark and it doesn't move very well. And like, my wife, who's a cyclist, like, after three years in menopause, you know, it's like her iron started to build, and it's not like, you know, we ate meat and so forth, and we really weren't paying over attention to this until recently. And I think she's someone who's had copper deficiencies her whole life.
RICK And so it's just, she was just primed for this to cause. And it's tough for her to give blood. So it coagulates, it's getting better. But every time you give some blood, you start moving that cycle. It's sort of this bicycle. It's important just to also think. It's like, well, you need to remove the blood, but you also need to add that natural vitamin a from grass fed dairy, butter, beef livers, or any livers that are natural a, which is different than palmitate or beta carotene. Yeah. That's not part of seroplasm. And your body has to convert them and it doesn't do it efficiently. So now we have this population which is deficient in not eating dairy. We're eating grass fed dairy that's deficient in c 15, you know, the fatty 15 from the dolphins that stabilizes the membrane and the mitochondria.
RICK And it's also deficient in vitamin a. So another piece to this puzzle is sort of been removed from our natural sources. So hemoglobin, iron, serum iron saturation, vitamin a, serum copper and seroplasm. The seroplasm, they're nice markers to have. Ideally, we would have. They're just going to give us a total amount. It doesn't give us an activity. If for some reason you can't easily get that, there's some labs that'll do that, you know, internationally, but there's just not available, which I don't understand, other than we're not supposed to know. Right. I don't know because they're doable. It's just no one does them. I'm not quite clear. So, yeah, so if people want to email me, we have this little sort of booklet on the mitochondrial protocol, you know, that sort of can go through some basic concepts and then has a page on.
RICK We created this for our athletes and patients and, you know, has a page on some of the markers and then it has sort of a terminology that helps show what's seroplasm, what hemoglobin is and what glutathione is and how each of these play a role on ferroxidase. If they want to learn a little bit more. Just email me, rick@purecleanperformance.com, and I'd be happy to send that. Give me motivation. I need to finish editing it, so maybe this will be done by the time you guys, it was pretty good. It was. Our editor, my wife, said he was the athlete, and we created it for, initially the cyclist, because she was coaching them, and she's like, no, this is too complicated. So we had to keep dialing it down.
FIONA So I want to also just divert a little bit to chronic kidney disease, because obviously, what happens in CKD is that erythroprotein EPO levels drop because that's produced by the kidneys. And then so we see a lot of anemia in chronic kidney disease due to low EPO levels. Now, is this going to extend across to that? Is the anemia that we're seeing in chronic kidney disease due to lower EPO and bone marrow not producing enough red blood cells? Is that true, or is it.
RICK I don't know. I asked Morley that as well, and he sent me some papers on oxygen sensing. There was actually an oxygen mechanism that's sensing the kidneys actually more than perhaps EPO. So to be honest, working with later stage kidney issues is something that I don't have a depth of experience to, but I do have experience in getting there. So part of that kidney, part of what caused the kidney issue, the diabetes, the uric acid, mitochondrial imbalances, the reactor is all iron and copper. I have a hard time in the story of my mother that the body is that there's not still tons of iron in there.
RICK My guess is to get it to move in patients with CKD. If you don't wait until your hemoglobin is a six. At some point, you hit a threshold where the dysregulation is causing such pathology that you, even if the fix is part of the problem, you still have to fix it. Right.
FIONA No, it totally makes sense. And it's such, because one of the biggest drivers we say of chronic kidney disease is inflammation and oxidative stress. And of course, it's happening in the small, fine, red blood cells in the nephrons inside the kidneys. And you go, well, of course. And I always talk about rusting from the inside out. It's quite a common thing. And so if we are rusting inside the nephrons and things like that from this copper, iron imbalance, then, you know, I can. That totally makes sense to fix that.
RICK Get iron as much as you can out of the tissues and, you know that there's excess iron. You know, this inflammation is visceral fat. Signs that there's excess iron is liver. In the US, there's clinics. You can do MRIs that actually look at iron in the liver. That's a helpful sense. Like I said, it can miss it. It could be in the spleen. But if you're seeing iron in the liver, you know, you're way overloaded with iron already. Then I default. Like, let's stop with all the nuances. Like, just give blood. No one says, just go to Red Cross and donate some blood. It's a good thing.
RICK As long as you're not to the point where it's so low already, donating some blood. As long as you fit their criteria, it's a good thing to do. You help people, and you're also benefiting yourself. You're offloading some extra iron.
RICK And it's also really easy to not get enough copper.
FIONA Fascinating. So to sum up for people listening (or reading!), because again, people are going to be pulling their bloods out and going, heh. So really, we. Hemoglobin, low end of normal range. You don't want a really high hemoglobin. You don't want it tanked into the bottom, but you want it in that lower end of normal. You're looking for your iron stores again. And we've got different reference ranges in Australia, but, you know, again, just in the normal range, you know, sort of sitting in that low.
RICK Iron levels in the, you know, sort of that smack of the mid range is where you want it.
FIONA And then, your saturation. Yeah. And then ferritin. Take that bad boy off the table. Like, let's ignore ferritin because in Australia that is what we look at. So let's ignore that. We're looking then maybe at total.
RICK It's a nuance. It's something to look at. If you're trying to figure out, like, this seems like an iron dysregulation and it could tell us if it's a spleen problem and it's more of a nuance. But to true iron status, ferritin you take out.
RICK There is also too much attention to zinc, if I have concern with zinc in my patients, I just tell them to have some nuts, you know, I just, I won't add it in, you're getting zinc from meat if you're eating meat and you're getting zinc from, you know, Brazil nuts and selenium. So I'm less concerned with those because zinc will deplete or can counterpose copper, especially in absorption. And that's much more of a concern in my viewpoint for people.
RICK Another point to touch on it how rapamycin seems to work and with this iron dysregulation, and I see it in athlete. You can use phlebotomy and you can use polyphenols such as curcumin or turmeric or, you know, ECGC. Yeah. Or solomerin or any of these polyphenols will block iron. And so, you know, whenever we eat meat, we'll have, we'll take some curcumin or green tea or coffee. You know, we're not, you know, things that'll block iron or lectins as well, or some dairy some yogurt or some kefir after mint will actually block the absorption as the lactoferrin in the dairy that will bind up. So there's some nutrients as well that can help, especially if you can't give blood. But there's just an additional benefit to giving the blood.
RICK Also higher intensity training or altitude hypoxia, oxygen training, where you're think about what do you need when you're at higher altitude? What do you need when you're performing higher? You need oxygen. So your body is going to make more red cells and it's going to require hemoglobin. So as long as you're not overfeeding iron, where's it going to get it? The tissues. So if you pull it out and then you're doing physical activity, you're now stimulating the body to pull iron out of the tissues. As long as you're not overloading it with the diet or you're someone who has the hemochromatosis genes, then you have to even be more aware, and those tend to be more sort of interesting. Western European based. That's where that enzyme is. And it goes back to the plague.
RICK There was something about the people who survived the plague. This particular gene had a benefit in supporting their survival. So that gene, which has a particular risk carried through in western European descent, sort of like sickle cell anemia, protecting against malaria, it carried through, you know, so now we're left with this remnant, you know, of a past time that doesn't provide that benefit that it did during this crucial time.
FIONA Fascinating. And I mean, I always say to anyone, don't go shoving a whole pile of copper supplements in there unless you've got some tests and you're working with a practitioner. But are there forms of copper that are better than others? Like if someone is going to supplement a doctor's or a naturopath or an integrative physician's going to prescribe that, is there a type? You know, we're looking at different types of eyes.
RICK We focus on magnesium glycinate. You know, we use copper glycinate or, you know, it used to be able to use beef liver, but it's not, it's just not there. We'll use some beef liver extracts or beef liver just for some of the nutrients, you know, the a and the b vitamins in there. Whatever's copper is there. Olive oil is a natural, great source of natural vitamin a, and it gives you a little bit of food based d, so it's really more not overloading d as well, because d can sort of decrease hepcidin which will help you pick up iron. And there's some other nuances to high dose d. And that's another conversation.
RICK You have to look at all the pieces and like the restoration too. It's not just ideally, it's giving some blood, you know, it's. It's using dairy, grass fed dairy orange, so that if you get dairy that's yellowish and eggs that are deep orange, naturally they tend to be richer in a, you know, so it's olive oil, magnesium, copper, glycinate and some whole vitamin C is also like an amla, acerola, camu, sea buckthorn. Those are complex c and they actually have some copper in their. In the center of the molecule. So. So that's also a potentially a better option than just using it.
RICK It is a better option than using just a straight ascorbic acid.
FIONA And beta carotene and the plant based have to be converted to a. Again, they're the same. They're no good. You need really beef liver and cod liver.
RICK No, plants not good for this. But they're not going to for this particular purpose. It's not the food we used to eat.
RICK Go back 100 years. What did people eat? Where was uric acid, which is actually a marker of mitochondrial efficiency? It's not. Uric acid causes gout, it's. Uric acid is a metabolic disease marker. There's markers you can look at for mitochondrial health.
FIONA So increased uric acid, you'd say, is a dysregulation or the mitochondria aren't functioning properly.
RICK For most. Right. There's certainly genetic susceptibilities, but when I see healthy metabolic people, the uric acid sits at three and a half. If you go back 100 years, the natural uric acid level was three and a half, and now it's under seven. No, people didn't change the food we eat, the lifestyle we change. And I haven't been able to find hemoglobin markers from 100 years ago, but suspicion from what we've seen is it was lower too. So the ranges of hemoglobin have climbed with decreased copper and increased iron.
FIONA Fascinating. Wow. Wow. That's kind of. This has been so fascinating. I mean, it's been on my radar since you and I spoke. And I've obviously heard of Morley Roberts before. And it gets. Sometimes people will bring up, he'll get.
FIONA Yeah. Yeah. So I guess the big takeaway for people is don't get hung up on iron so much. I'm beginning to think, you know, it's a bit over prescribed in our population
RICK We are rusting 100% over prescribed in our population.
FIONA Yeah. And so really, if you have chronic low iron levels and you take supplementation and it doesn't improve, you need to go and work with an integrative practitioner that's maybe trained under Morley or understands the nuances that knows to look at some of these other markers. I'll put Doctor Cohen's email address in there if you're interested in his PDF handout. To really get a better understanding what those markers mean, you better get typing way in editing. I'll pop that down in the show notes so you can shoot him an email and he can send that information out and. Yeah. Thank you. Because I think this is an area that people really do get hung up on. And as I say, I just know it has been a naturopath.
FIONA You know, the thing that goes up every day into the naturopathic Facebook pages and stuff is this person's anemic. We're giving them iron. What? You know, like it's over and over again. So, yeah, it's good to take a step back. Yeah. We can't all be deficient. Like, it really cannot be that. So what else is going on? So. So thank you.
RICK Yeah, okay, my pleasure.
RICK One last thing, I think just to make sure you check all those markers to know you're an individual and to make sure you understand. Iron dysregulation is the problem for 99.9% of the people and not iron deficiency. So yes, you may be anemic, but it's not due to the lack of iron in your body. It's due to the lack of bioavailability of that mineral recycling process or the iron recycling process.
FIONA Fascinating. And then, I mean, a whole other topic. But I've got colleagues who do, who use leeches on things like arthritis. And I'm wondering now I'm like, was that just stored iron in the joint? And the leeches are just.
RICK Yeah, right, yeah. I mean, another way, like acupuncture, they do, wet cupping is another way that, you know, to pull out iron as well. It's sort of creepy, but same as the leeches.
FIONA Oh, love it. Well, thank you again for your knowledge. All the details are gone below. And if you want to know more about what we do, you can head to www.kidneycoach.com. Remember to hit click. Yeah, hit click like and subscribe. That way you will get notified anytime we put up new videos. Doctor Cohen, always appreciate your time and your knowledge. I always learn so much just sitting with you and we will definitely have you back! Thanks, Rick!